
Treating trigger points can be effective in easing, sometimes eliminating, muscular pain. What are trigger points, what causes them, and how can they be treated?
Trigger points are found in taught bands of muscle tissue. When palpated, a taught band feels like a thin rope or cord while a trigger point within the taught band can feel like a lump or knot. Local tenderness and pain referral is a common peculiarity of trigger points and helps to identify the focus of a treatment plan. With compression they will elicit pain or other sensation such as tingling, numbness, and (less likely) burning that refer to other areas of the body in a nonrandom typical pattern. Trigger point maps or charts show typical referral patterns. In their book Myofascial Pain and Dysfunction – The Trigger Point Manual (Volume 1), David Simons and Janet Travell (1999) define a myofascial trigger point:
A hyperirritable spot in skeletal muscle that is associated with a hypersensitive palpable nodule in a taught band. The spot is painful on compression and can give rise to characteristic referred pain, referred tenderness, motor dysfunction, and autonomic phenomena. (p.5)
Janet Travell (1901 – 1997) is recognized for clarifying trigger points and establishing the characteristic pain referral patterns. A cardiologist, she was also an associate professor at Cornell University Medical College where she lectured in clinical pharmacology. In her autobiography, Office Hours: Day and Night (1968), Travel shares with her readers her professional association with John F. Kennedy. Kennedy was a senator when he first met Travell. On hiatus from the senate due to severe back and leg pain, he was referred to Travell for treatment (p. 5). Clearly, Kennedy respected Travel for her abilities as a physician. Her autobiography describes her visits with him and his wife Jacqueline at their coastal home in Florida. His trigger point treatment was so successful that when he was elected president of the United States, he appointed Travell White House physician where she served during the Kennedy and Johnson administrations from 1961 – 1965 (p. 358). Following this, she published articles in medical journals and wrote her autobiography. She collaborated with David Simons in the writing of Myofascial Pain and Dysfunction – The Trigger Point Manual (volumes 1 and 2). Years after its publication, it remains a must read for anyone who wishes to delve into the world of trigger point therapy. The illustrations are worth the purchase of the book alone – though it is also full of valuable information.
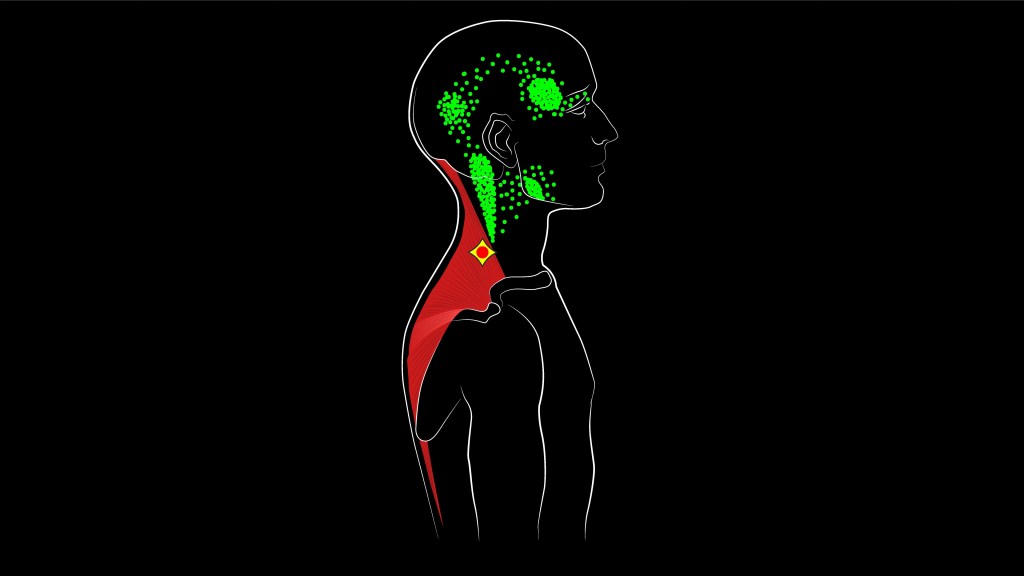
Active trigger points refer pain even when pressure is not being applied to the area. For example, active trigger points in the infraspinatus muscle (originating at the infraspinous fossa of the scapula and inserting at the greater tubercle of the humerus) can refer pain in the anterior shoulder as well as the anterior and lateral arm and forearm. The image above shows the trapezius muscle (upper). The red mark within the yellow diamond shape shows the trigger point location. The green dots indicate the pain referral areas. Pain might be felt during certain movements or positions, activities during the day, or without an apparent stimulus. When compression is applied to the active trigger point, it will reproduce the pain pattern experienced during the course of a day. Satellite trigger points occur in associated muscles or that are in the referred pain zones of the primary trigger point. By treating the primary, the satellites often will cease being a problem. When a therapist applies pressure on a latent trigger point, it may come as a surprise to the client that they feel referred pain. This is because latent trigger points do not cause pain except with manual pressure on the trigger point. However, they “often cause motor dysfunction (stiffness and restricted range of motion) and are more prevalent than active TrPs” (Simons, Travell, 1999, p.12). While it is important to treat the active trigger points to help decrease or resolve symptoms, it is also beneficial to address latent trigger points as they can affect muscle function. Additionally, they could become active at some point if left untreated. In addition to referred and local pain, trigger points can cause muscle spasms, reduced range of motion, weakness, and motor dysfunction.
Trigger points can be caused by injury such as falls and car accidents; even an inactive lifestyle. Another cause is repetitive movements such as texting, typing, sport activities, playing a musical instrument. This is especially true if activities such as these are performed with body mechanics that are in need of improvement. Poor posture and a prolonged state of shortened contraction can be a factor in the development and continuation of trigger points. For example, sitting slumped with rounded shoulders and pushing the head forward and up to view the computer screen can cause trigger points to develop in the front of the chest as well as the back of the neck and head region. While pain may be felt in the upper back, muscles in this area – rhomboids and mid trapezius – are lengthened and weak. While this area can be addressed, it will be most important to treat the shortened muscles – in this case, pectoralis major. Additionally, treating trigger points in the posterior cervical muscles can bring pain relief and improve muscle function.
Travel and Simons largely show a spray and stretch method for treatment of trigger points. A vapocoolant is used “while the muscle is being extended gently to its full stretch length” (p. 127). Other methods are effective and perhaps generally safer. Manual therapy uses a compression technique as well as slow, short gliding strokes. There are other methods such as dry needling , injection, and self massage tools. During a treatment session, passive stretching may follow the deactivation of a trigger point. Stretching can be done by the client on their own some time during the day following treatment.
Manual therapy is best defined by Travel and Simons, ‘Trigger Point Pressure Release’ is an “Application of slowly increasing, non painful pressure over a trigger point until a barrier of tissue resistance is encountered” (p. 8). From there, as tissue releases, slowly increase pressure as tension melts and releases. Receiving trigger point therapy should not be a painful experience. Pain is neither necessary or helpful. On a scale from one to ten, the pain level perceived by the client should not exceed a six. Five is a good level of intensity. While receiving, it can be helpful to have the intention of releasing and letting go of mental or physical tension.
Self care: Besides the years of education and experience a professional therapist has to offer, receiving treatment from a therapist allows the client to experience a relaxed state while trigger points are addressed and muscle tension is eased from the body. Additionally, it’s always favorable when someone else can work on those harder to reach areas. However, following successful treatment, it is beneficial to learn how to self treat trigger points. To do this, grab a self help book. Suggested: 1). The Trigger Point Therapy Workbook: Your Self-Treatment Guide for Pain Relief by Clair Davies and Amber Davies 2).The Concise Book of Trigger Points: A Professional and Self-Help Manual by Simeon Niel-Asher. My recommendation is to augment self help sources with the book Myofascial Pain and Dysfunction: The Trigger Point Manual (volume 1 and 2) by David Simons and Janet Travell. Also recommended is a book on anatomy; however, there are good online sources.
Increasing body awareness and gaining an understanding of the cause can help trigger point pain from returning. If work or a favorite activity is contributing to the pain, yet must continue, it will be important to assess body mechanics and one’s work station and make necessary changes. Our bodies are always under stresses no matter how in tune with our bodies we are. Every so often during the day take opportunities to stretch, strengthen, and move. Stretching: Breathe into the stretch and have the intention of lengthening. Standing meditation can also be valuable as it reminds the body to align physically and energetically. Standing parallel with feet about hip width apart, drop the pelvis down towards the floor, open the chest, and bring the shoulders gently back, paying attention to correct any rounding of the shoulders. Then, draw the head and ears back in line with the open shoulders. Bring attention to the breath for a short meditation. Attention can also flow to each of the seven chakras. Notice if this makes a difference to a sense of alignment. If time allows, I like to follow the stretch and strengthening exercises with lying meditation and deep relaxation.
